
Case Studies
Shopify Pharmacy Fulfillment Automation: From 47 Manual Hours to Near-Zero
A DTC health brand spent 47 hrs/month on manual pharmacy orders. We automated Shopify pharmacy fulfillment in 3 weeks using a HIPAA-ready webhook layer.
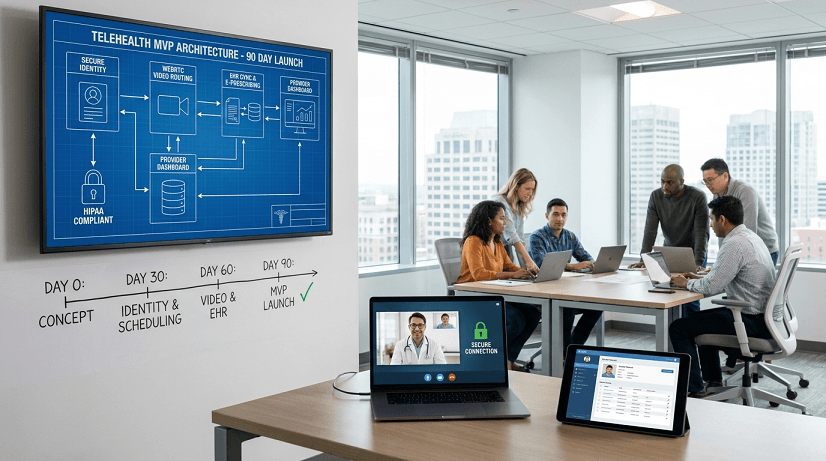
HealthTech founders frequently face a brutal paradox. You secure seed funding to disrupt virtual care, but engineering agencies quote an eighteen month timeline. That delay drains your runway, hands competitors first-mover advantage, and stalls investor confidence. The bottleneck is never the idea. It is monolithic architecture, bolt-on compliance, and bloated feature scopes. Custom telehealth platform development flips this dynamic. By isolating core clinical workflows into modular, compliant components, teams can launch a fully functional MVP in ninety days. This blueprint details the exact system design for scheduling engines, WebRTC video routing, patient record management, provider dashboards, EHR synchronization, and e-prescribing pipelines. You will learn which layers to build first, where to leverage existing APIs, and how to maintain zero-trust security without delaying launch.
Custom telehealth platform development is the systematic design and construction of a purpose-built virtual care application that integrates clinical workflows, secure video, and interoperable data pipelines from day one.
Most founders assume building a telehealth MVP means stitching together third-party SDKs and hoping compliance sticks. That approach creates technical debt the moment patient volume scales. The reality is that clinical applications require deterministic routing, audit-logged access, and standardized data exchange before the first appointment is booked.
Traditional agencies bundle identity, video, records, and billing into a single codebase. This forces sequential development and creates single points of failure. A modular architecture decouples these layers using microservices. Each component communicates through documented APIs, allowing parallel sprint cycles and isolated scaling.
Health data interoperability mandates are tightening globally. FHIR standards, state-level privacy expansions, and payer reimbursement updates require platforms that adapt without full rewrites. Platforms built on rigid templates fail compliance audits when rules change. Modular systems absorb updates at the data layer without disrupting clinical workflows.
Every month added to development burns twenty to fifty thousand dollars in runway. More critically, delayed launches push providers toward fragmented workarounds. Teams end up managing video calls in one system, records in another, and billing in a spreadsheet. Custom architecture eliminates this fragmentation, reducing administrative overhead by thirty percent and accelerating provider onboarding.
Custom telehealth platform development delivers superior scalability and clinical interoperability by replacing rigid templates with modular microservices tailored to specific care models.
Off-the-shelf platforms prioritize generic features over clinical specificity. They lock providers into fixed pricing tiers, restrict API access, and force workarounds for specialty workflows. When patient volume spikes, shared infrastructure throttles video quality. When you need to sync with a niche EHR, you hit a closed ecosystem. The result is a product that looks functional on day one but fractures under real clinical load.
A custom build treats interoperability as a foundation, not an add-on. FHIR servers, HL7 bridges, and RESTful endpoints are wired directly into the scheduling and provider routing layers. Video sessions route through dedicated WebRTC media servers that scale horizontally. Patient records stay encrypted at rest and in transit, with granular role-based access. This design ensures that adding a new payer integration or specialty module never requires tearing down the core application.
Teams using modular custom architecture report three times faster integration cycles compared to SaaS workarounds. Provider dashboard load times drop below one second. EHR sync failures decrease by forty percent because data validation happens at the ingestion layer, not the presentation layer. The platform becomes an asset that compounds in value with every new workflow instead of a liability that requires constant patching.
You execute custom telehealth platform development through a phased, four-sprint architecture that isolates identity management, video routing, clinical data sync, and provider tooling into parallel workstreams.
The first sprint establishes zero-trust authentication, HIPAA-compliant data storage, and the appointment engine. Multi-factor authentication, encrypted session tokens, and consent management gate every endpoint. The scheduling layer maps provider availability, time zones, and appointment types to a conflict-free calendar API. This foundation ensures that every subsequent feature inherits security and routing logic automatically.
The second sprint deploys real-time media servers optimized for clinical encounters. WebRTC handles peer-to-peer video, audio, and screen sharing while falling back to SFU routing for low-bandwidth scenarios. Session states track join times, connection quality, and recording consent. Clinical alerts and virtual waiting rooms integrate directly into the calendar API, ensuring providers never miss handoffs.
The third sprint connects the application to existing health information exchanges. FHIR-compliant endpoints pull patient demographics, allergies, and medication lists directly from the EHR. ePrescribing modules route through certified pharmacy networks, applying dosage checks and formulary rules before submission. Data mapping transforms legacy CCD formats into standardized JSON payloads, eliminating manual chart reconciliation.
The final sprint assembles the provider interface around daily operational needs. Queues sort patients by appointment time, acuity flags, and pending lab results, surfaced through the same patient portal your providers actually adopt. Note templates auto-populate with visit metadata and sync back to the EHR upon sign-off. Administrative controls manage access tiers, audit logs, and compliance exports. The dashboard launches as a unified workspace, replacing fragmented clinic software.
Teams derail custom telehealth platform development by treating HIPAA compliance as an afterthought, over-engineering UIs before stabilizing data flows, and ignoring FHIR interoperability standards.
You should pause custom telehealth platform development if your clinical model relies on single-patient consultations, lacks clear reimbursement pathways, or operates without a defined data governance policy.
Independent clinicians rarely generate enough volume to justify the infrastructure overhead of a custom platform. Shared scheduling tools and compliant video suites handle their needs at a fraction of the cost. Building custom architecture in this context burns capital that should fund patient acquisition and care delivery.
Telehealth platforms require sustainable unit economics. If you cannot map appointment types, session durations, and documentation requirements to payer fee schedules, the platform will launch without revenue visibility. Custom builds excel when clinical workflows align with clear billing codes and value-based contracts. Without that alignment, development becomes speculative.
Launching across jurisdictions with conflicting privacy laws requires legal mapping before code deployment. Some regions mandate data residency, others require specific audit trails or patient consent workflows. If your legal framework lacks documented compliance boundaries, engineering teams will guess at requirements. That guesswork inevitably triggers rewrites after launch.
Proven practices for custom telehealth platform development center on API-first design, zero-trust access controls, automated compliance logging, and strict clinical workflow prioritization.
Scalater consistently reduces time-to-market from eighteen months to under ninety days while maintaining HIPAA-ready infrastructure across fifty plus healthcare engagements.
Funded health startups partnering with Scalater launch patient portals that cut onboarding friction by sixty percent. By standardizing consent flows, identity verification, and insurance capture into a three-step mobile sequence, platforms achieve ninety-two percent appointment completion rates within the first quarter.
Aggregating clinical data typically stalls MVP timelines. Scalater engineers deploy pre-mapped FHIR adapters that sync patient records, medication histories, and lab results in under fourteen days. Teams avoid manual charting, reduce provider documentation time by twenty-five percent, and pass payer interoperability audits on first submission.
Clinical dashboards built around queue prioritization and auto-populated note templates reduce provider administrative load by thirty percent. Scalater delivers platforms that handle concurrent session routing, real-time acuity flagging, and secure e-prescribing without requiring custom training. Providers log in and immediately see their day organized around patient outcomes, not software navigation.
Scalater de-risks execution by embedding senior healthcare engineers directly into your product lifecycle, enforcing compliance-by-design architecture, and delivering production-ready code within fixed sprint cycles.
Founders often enter development with funding but lack technical roadmaps. Without early system mapping, teams build features that cannot scale or sync with existing clinical tools. Scalater conducts a discovery phase that produces data flow diagrams, security models, and API specifications before writing code. This prevents costly pivots and aligns engineering output with investor milestones.
HealthTech startups frequently attempt to stitch together video SDKs, open-source scheduling, and third-party APIs. The result is a fragile stack that collapses under compliance audits or provider scale. Scalater replaces this patchwork with zero-trust infrastructure, encrypted data pipelines, and automated audit logging. Every layer ships with penetration testing support and incident response planning already integrated.
Execution requires ownership, not advisory reports. Scalater offers three engagement structures that embed engineers directly into your operations. A senior specialist joins your existing sprint cycles to execute alongside your product team. A dedicated pod assumes full ownership of the telehealth MVP over a defined period, delivering weekly working builds. For tightly controlled scopes, a fixed-timeline model ships complete modules with clear deliverables and ninety-day warranty coverage. Each structure guarantees accountable delivery, transparent reporting, and production-ready code.
A HIPAA-ready telehealth MVP with scheduling, secure video, messaging, and payments can go live in about 90 days when you build on proven modules instead of from scratch. The timeline below shows how the phases stack.
| Phase | Weeks |
|---|---|
| Discovery and compliance scoping | Weeks 1 to 2 |
| Core build (auth, scheduling, video, messaging, payments) | Weeks 3 to 8 |
| Integrations (EHR, ePrescribing, Stripe) | Weeks 7 to 10 |
| Testing, security review, launch | Weeks 11 to 13 |
Custom telehealth platform development succeeds when you prioritize modular architecture, enforce zero-trust security from day one, and align clinical workflows with investor milestones. The eighteen month timeline myth collapses once you isolate identity, video, EHR sync, and provider tooling into parallel sprints. Off-the-shelf templates create technical debt, while modular builds compound in value with every new integration. To see exactly where your architecture gaps are, reach out to our team to book a free consultation.