Shopify Pharmacy Integration
The Shopify to Pharmacy, EHR and ePrescribing Integration Guide
Shopify pharmacy integration routes orders to pharmacy, EHR, and eRx systems without exposing PHI. Learn the compliant middleware pattern.
Clinical data silos continue to delay care delivery and inflate integration costs across hospital networks. When patient records, lab results, and billing systems operate on disconnected schemas, engineering teams waste months building fragile point-to-point connectors. Ignoring these structural gaps creates compliance exposure, slows provider workflows, and blocks scalable telehealth expansion. Structured healthcare api development solves this fragmentation by replacing custom endpoints with standardized, interoperable data pipelines. This guide covers FHIR resource modeling, protocol selection, version control strategies, and documentation standards that keep clinical systems compliant and performant under real-world load.
Healthcare api development transforms disconnected medical databases into interoperable, audit-ready networks that comply with federal data exchange mandates. Modern clinical workflows require real-time synchronization between electronic health records, laboratory information systems, and remote monitoring platforms. Traditional data sharing methods rely on batch processing and proprietary formats that cannot support on-demand care coordination. Regulatory bodies now enforce standardized exchange rules that mandate machine-readable clinical data. Organizations that fail to adopt structured API architectures face delayed reimbursements, interoperability penalties, and mounting technical debt.
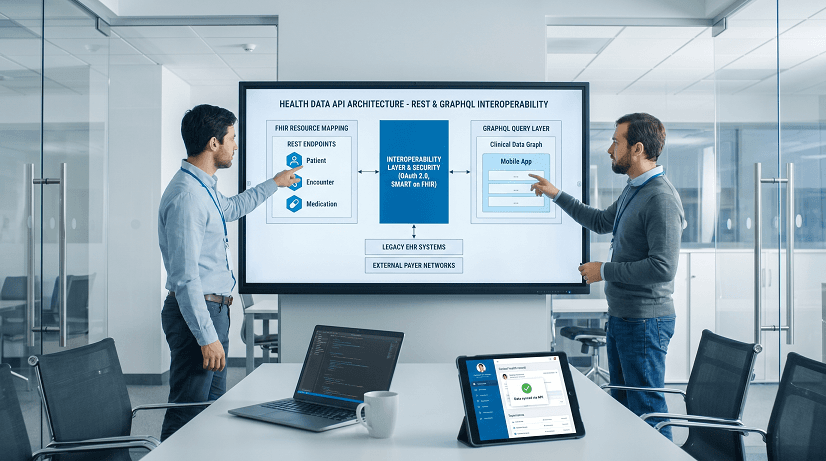
HL7 FHIR resources replace ad hoc JSON schemas with clinically validated data models that map directly to patient demographics, conditions, medications, and observations. Teams building custom REST payloads often duplicate clinical terminology and lose semantic context during transmission. FHIR structures embed ValueSet bindings, reference links, and extension hooks that preserve medical accuracy across systems. This standardization eliminates manual mapping layers and reduces integration testing cycles by nearly half.
The Centers for Medicare and Medicaid Services and ONC now require provider networks to enable patient data access through standardized APIs. Payer-provider interoperability rules mandate timely claims and coverage data sharing. Health systems that rely on legacy EDI transactions or manual portals cannot meet these deadlines. API-first architectures satisfy compliance requirements by exposing versioned endpoints, enforcing OAuth 2.0 scopes, and maintaining immutable audit trails for every data request.
Unstructured data pipelines trigger audit failures when clinical records move without proper consent tracking or encryption in transit. Hospital IT departments frequently spend six to nine months troubleshooting broken HL7 feeds and mismatched patient identifiers. These delays increase liability exposure and block revenue cycle automation. Structured API development prevents these bottlenecks by embedding security controls, consent flags, and data validation rules directly into the transport layer.
Healthcare api development consolidates scattered medical records into unified query pathways that reduce latency, enforce security boundaries, and support multi-system synchronization. Legacy integrations force engineering teams to maintain dozens of custom connectors that break when source systems update their schemas. API architecture centralizes data routing, applies consistent validation logic, and exposes predictable response formats for downstream applications. This shift replaces fragile point-to-point links with scalable, self-documenting networks.
SOAP-based clinical integrations rely on rigid XML envelopes and WSDL contracts that resist rapid iteration. Custom REST endpoints often expose inconsistent field names, unpaged result sets, and missing error codes. These designs force frontend teams to implement workarounds for missing patient identifiers, unnormalized lab values, and unpredictable response shapes. Maintenance costs scale linearly as more systems connect to the same unstandardized endpoints. Debugging production failures becomes nearly impossible without structured logging and versioned contracts.
GraphQL allows clinical applications to request exactly the patient demographics, medication histories, and care team assignments required for a specific screen. FHIR-compliant GraphQL servers translate nested queries into optimized database joins while preserving access control rules. This approach eliminates over-fetching in mobile health apps and reduces network payload sizes by 40 to 60 percent. Teams retain REST endpoints for webhook subscriptions, bulk exports, and regulatory reporting where predictable stateless operations remain necessary.
Healthcare api development requires phased implementation that prioritizes resource modeling, version control, and machine-readable documentation before exposing endpoints to production traffic. Engineering teams must define clear boundaries around clinical data ownership, establish deprecation timelines, and validate schema compliance against official FHIR implementation guides. Skipping these steps leads to breaking changes during system upgrades and compliance audits.
Start by mapping clinical use cases to core FHIR resources like Patient, Encounter, Condition, and MedicationRequest. Establish explicit reference chains that link encounters to patients and medications to prescribing providers. Use contained resources for inline data that lacks independent audit value. Apply search parameters and composite criteria to filter results without requiring full resource downloads. This structure prevents circular references and keeps response payloads predictable.
Embed semantic versioning in endpoint URLs and maintain backward compatibility across minor releases. Publish a public deprecation schedule that spans at least two release cycles before removing fields or changing response structures. Use HTTP headers to warn consumers about upcoming changes and route legacy requests to compatible adapters. This approach prevents sudden frontend failures and gives integration partners time to update their clients.
Document every endpoint using OpenAPI 3.0 or 3.1 with explicit request schemas, response codes, and authentication scopes. Include FHIR resource profiles, extension definitions, and pagination rules directly in the specification files. Validate the specification against clinical data samples before deployment. Automated testing pipelines can parse these files to generate mock servers, client SDKs, and compliance reports without manual intervention.
Healthcare api development fails when teams expose unversioned endpoints, ignore reference integrity, or skip security scoping during initial design. These mistakes create fragile integrations that break during system updates and trigger compliance violations.
Healthcare api development is not the right approach when your architecture serves isolated internal workflows or relies on fixed-schema legacy systems that cannot expose structured data. Forcing API patterns onto incompatible environments creates unnecessary overhead and delays core functionality.
Older electronic medical record systems store clinical data in rigid relational tables that lack export hooks or standardized identifiers. Attempting to wrap these databases with modern API layers requires extensive data migration, schema translation, and continuous synchronization. Organizations should prioritize database modernization and ETL pipelines before investing in real-time API infrastructure.
Staff scheduling dashboards, inventory trackers, and facility maintenance portals rarely require interoperable clinical data exchange. Building standardized API contracts for these systems adds unnecessary security overhead, documentation maintenance, and version control complexity. Direct database access or internal service calls remain more efficient when external integration is not required.
Healthcare api development succeeds when teams enforce strict data contracts, automate compliance validation, and align endpoint design with actual clinical workflows. Generic API patterns fail in healthcare because medical data requires semantic accuracy, auditability, and role-based access control.
Scalater consistently reduces clinical data sync delays and accelerates third-party integrations by replacing custom connectors with standardized, versioned API architectures. Our engineering teams focus on FHIR-compliant data models, secure query optimization, and automated documentation that scale across hospital networks and payer platforms.
We have deployed interoperable API layers that synchronize patient demographics, care plans, and lab results across multiple EHR vendors without manual mapping. These integrations reduce data reconciliation cycles from weeks to hours and eliminate duplicate record creation. Provider networks report faster care coordination and fewer scheduling conflicts after consolidating fragmented patient profiles into unified API pathways.
Migrating legacy REST endpoints to FHIR-optimized structures and selective GraphQL queries cuts average response times by 40 to 65 percent. Clinician- and patient-facing applications load complete medication histories, allergy alerts, and recent encounters without multiple sequential requests. This reduction in network overhead directly improves provider satisfaction and decreases time spent waiting for system responses during patient visits.
Scalater embeds directly into your engineering workflow to design, secure, and deploy interoperable clinical APIs that meet regulatory standards and scale under real-world traffic. We focus on execution, architectural safeguards, and production-ready documentation that keep your integrations stable through system updates and compliance audits.
Healthcare organizations frequently stall when mapping legacy HL7 v2 messages to modern FHIR resources or configuring multi-tenant security layers. Teams escaping a black-box vendor can follow our telehealth platform migration playbook for a zero-downtime cutover. Our engineers join your existing sprint cycles to audit current data flows, implement reference chaining, and configure OAuth scopes aligned with SMART on FHIR requirements. This hands-on collaboration prevents compliance gaps and ensures endpoints pass third-party security reviews.
Teams building clinical APIs without specialized guidance often expose inconsistent schemas, skip deprecation windows, or mix REST and GraphQL patterns without clear boundaries. We deploy dedicated engineering pods that own specific API outcomes, from specification generation to load testing. This model isolates integration risks enforces version control discipline, and delivers production endpoints on fixed timelines.
Scalater structures engagements around clear deliverables that align with your release calendar and compliance deadlines. We establish fixed-scope milestones for resource modeling, security configuration, and OpenAPI documentation, then transition ownership to your internal teams. This approach eliminates advisory-only handoffs and ensures your API infrastructure operates reliably after deployment.
Healthcare api development succeeds when teams prioritize standardized data models, enforce strict version control, and align endpoint design with actual clinical workflows. FHIR resource mapping eliminates custom schema duplication while GraphQL and REST serve complementary roles based on query complexity and compliance requirements. Documenting endpoints with machine-readable OpenAPI specifications prevents breaking changes and accelerates partner onboarding. To map out your exact integration path and avoid costly architectural missteps, reach out to our engineering team to book a free consultation.

Shopify pharmacy integration routes orders to pharmacy, EHR, and eRx systems without exposing PHI. Learn the compliant middleware pattern.

Adding AI to a healthcare platform later triggers a full rewrite. These 6 architecture choices keep your roadmap at 3 months, not 3 years.

Most patient portals go underused because teams skip provider workflow design. Here are the five traits that separate portals clinicians adopt from portals they ignore.